NECK DISSECTION (Removal of Cancerous Neck Lymph Nodes)
 Your surgeon at Suburban Ear, Nose, and Throat has extensive training in the treatment of head and neck cancer. Part of that treatment includes surgically removing lymph nodes in the neck. The formal name for this operation is called a neck dissection. Each side of the neck contains 20-100 lymph nodes. Lymph nodes, commonly referred to as "glands," are a part of the immune system. Lymph nodes act as a "filter" for conditions of the head and neck. They may enlarge in response to infection, inflammation, and tumors. Malignant (cancerous) tumors of the head and neck can sometimes spread (metastasize). The site of origin of the cancer is called the primary tumor, and any spread of cancer to other sites is called metastasis. The first place that head and neck cancers will typically metastasize is to the lymph nodes of the neck. They can even develop tumors of their own called lymphoma.
Your surgeon at Suburban Ear, Nose, and Throat has extensive training in the treatment of head and neck cancer. Part of that treatment includes surgically removing lymph nodes in the neck. The formal name for this operation is called a neck dissection. Each side of the neck contains 20-100 lymph nodes. Lymph nodes, commonly referred to as "glands," are a part of the immune system. Lymph nodes act as a "filter" for conditions of the head and neck. They may enlarge in response to infection, inflammation, and tumors. Malignant (cancerous) tumors of the head and neck can sometimes spread (metastasize). The site of origin of the cancer is called the primary tumor, and any spread of cancer to other sites is called metastasis. The first place that head and neck cancers will typically metastasize is to the lymph nodes of the neck. They can even develop tumors of their own called lymphoma.
After malignant cells have been growing in a lymph node for some time, the lymph node/s enlarge. The nodes can often then be identified on exam, or by one or more types of diagnostic imaging (CT scan, MRI, or PET scan). Depending on the staging (extent) of your head and neck cancer, a neck dissection might be recommended as part of your treatment plan. Neck dissection might be suggested early in the therapy or towards the end of your cancer treatment, depending on your particular circumstance. We might recommend neck dissection even if there is no evident spread into your lymph nodes on exam or imaging. This is done to help us determine if there has been microscopic metastasis. The presence of microscopic metastasis would then have significant implications in guiding what other treatments are necessary, e.g. radiation or chemotherapy.
There are several types of neck dissections, and the particular type of surgery depends on your individual cancer. We will talk to you about whether or not it will be possible to preserve certain anatomic structures in your neck, depending on the type of neck dissection that your situation dictates. Sometimes the neck dissection is performed upon both sides of the neck. Often, the neck dissection is performed in conjunction with other surgery to remove the primary tumor also. The primary tumor can be anywhere in the head and neck, including the tongue, tonsils, throat, larynx (voice box), or other sites. Each individual situation is unique, and we will help you understand all the specifics of what we have recommended to you.
In general three types of neck dissection are performed:
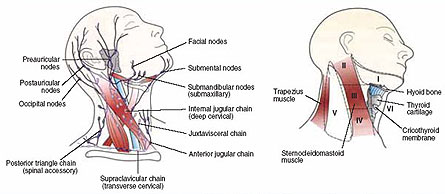
Selective Neck Dissection: Only certain groups of lymph nodes will be removed. There are 6 lymph node regions in your neck as demonstrated in the diagram above. With a selective neck dissection, several lymph node regions will be removed, depending on the location of your primary tumor. Usually this type of neck dissection is recommended in three situations: (1) to determine if there has been microsopic spread of your cancer, (2) to determine if all the cancer cells are gone after radiation and/ or chemotherapy, or (3) to remove a small malignant lymph node if surgery is the only treatment and no chemotherapy or radiation therapy is planned.
Modified Radical Neck Dissection: Most of the lymph nodes from the neck (from the jawbone to the collar bone) will be removed, along with either a muscle, nerve or vein (or combination of 2 of these structures). This type of neck dissection and the below described radical neck dissection are performed when there is evidence of more extensive involvement of lymph node metastasis.
Radical Neck Dissection: Nearly all of the lymph nodes from the neck will be removed, along with a muscle (sternocleidomastoid muscle), a nerve (cranial nerve XI — spinal accessory nerve), and a vein (internal jugular vein). It is important to understand that it is generally safe to remove these structures without causing significant bodily dysfunction or deformity.
Before your operation, your surgeon at Suburban Ear, Nose, and Throat will explain the type of neck dissection you are going to have. The surgery is guided by the size and location of the involved lymph nodes in your neck. During the operation, the surgeon will make an incision in your neck, which begins just below your ear and extends downward towards the center of your neck. This will provide exposure to the lymph nodes in your neck. Occasionally, the surgeon may also remove other tissues such as a portion of skin, if it is affected by the tumor.
The indications and risks of surgery must be understood prior to proceeding with surgery. Alternatives to surgery including radiation therapy and/or chemotherapy will be discussed before proceeding with surgery.
2 WEEKS PRIOR TO SURGERY: Strictly avoid all anti‐inflammatory drugs for two weeks pre‐operatively. This includes aspirin, Advil, ibuprofen, Naprosyn, Celebrex or any other non‐steroidal anti‐inflammatory drug (NSAIDs). These medicines increase your risk of bleeding. These medicines must also be avoided for at least one week after surgery. Tylenol (acetaminophen) is not an anti‐inflammatory so it is fine to take.
NIGHT BEFORE SURGERY: No solid foods (that includes milk, cream etc.) for 8 hours prior to surgery. Typically this means no solid foods after midnight before the surgery. Small volumes of clear liquid may be drank up to 4 hours prior to surgery (examples: water, tea, Gatorade, or coffee with NO milk or cream).
HOSPITAL STAY: Patients who undergo neck dissection will usually be admitted to the hospital for 2-5 days. They will usually spend the first night in the intensive care unit for observation.
LAB WORK: Your physician may request that blood work is done prior to surgery. If this is needed, you will receive an order form for this blood work, and the location of the lab to perform the blood draw is usually recommended based on your insurance company and where your surgery is to be performed.
SURGICAL RISKS AND POSSIBLE COMPLICATIONS:
Despite neck dissection having many potentially serious risks, they occur very infrequently, and the surgical procedure is usually performed without difficulty. Although substantial tissue involved with cancer is removed from the patient’s neck, this operation does not generally lead to a dramatic degree of disfigurement or dysfunction.
BLEEDING: significant bleeding is rarely encountered during neck dissection surgery. Despite this, there is a small chance of excessive blood loss possibly requiring transfusion. If carotid artery injury was to occur you may suffer a stroke, or this could be a fatal event. This injury is extremely rare.
There are multiple nerves in the head and neck that are exposed during neck dissection surgery, and therefore, placed at risk during the surgery:
Marginal mandibular nerve: injury to the marginal mandibular branch of the facial nerve can lead to temporary or permanent facial weakness to the lower lip on the surgical side.
Spinal Accessory Nerve: depending on the type of neck dissection performed, you may have temporary or permanent weakness to your shoulder. Sometimes it is required that the spinal accessory nerve be removed as a planned part of the neck dissection in order to optimize eradication of the cancer. The spinal accessory nerve gives strength to your shoulder muscles, allowing shrugging and full raising of your arm. Shoulder pain can occur after removal of this nerve, but it can be managed with post-operative physical therapy. Even when the spinal accessory nerve is preserved, up to 50% of patients may experience temporary shoulder weakness and/or discomfort.
Vagus nerve: Injury to the vagus nerve, though extremely rare, will result in hoarseness, swallowing troubles or throat dysfunction after surgery.
Phrenic nerve: One half of your diaphragm may be paralyzed if the phrenic nerve is injured during surgery. This is an extremely rare injury. Although in many cases, injury to one of the phrenic nerves is not that symptomatic, it can lead to chronic shortness of breath.
Lingual nerve: Injury to the lingual nerve will result in numbness to one half of your tongue, but the tongue will have normal mobility.
Hypoglossal nerve: Injury to the hypoglossal nerve will cause weakness or paralysis to one half of the tongue. The tongue will retain normal sensation. Some slurred speech can be initially expected, but with speech and swallowing therapy, normal or near-normal function can be re-established.
CHYLE LEAK: On occasion, larger lymph vessels are encountered during surgery. Care is taken to prevent leakage of lymph fluid; however, if this occurs post-operatively, it may require a period of time after surgery where you are only fed with IV fluids in order to facilitate resolution of this leak. In addition, when food is introduced, it may be a modified diet for several weeks. Rarely, further surgery may be required to control this problem.
SWELLING: patients may notice intermittent, but long-term swelling of the skin of the face and neck after undergoing neck dissection. This can be improved by sleeping upright for a couple of nights.
Poor scarring or poor healing can occur, especially if you have already received radiation therapy. On occasion further surgery is necessary to correct this problem.
With most neck dissections, one or more sensory nerves are removed during the surgery. Removal of these nerves is a planned part of the neck dissection, and does not represent a complication. In addition, it does not alter one’s appearance. It will likely result in numbness to the ear, neck, and/or shoulder skin.
Your operation will be carried out under a general anesthetic. As with any type of surgery, the risks of anesthesia such as drug reaction, breathing difficulties and even death are possible. Please feel free to discuss any specifics of the anesthesia with your anesthesiologist.
All efforts are taken by the physicians of Suburban Ear, Nose, & Throat Associates, as well as your other physicians, to attempt to cure you of your head and neck cancer. There is a realistic chance of recurrence of your cancer over time. The chance of tumor recurrence is directly related to the size and stage of your cancer, as well as the biological aggressiveness of your tumor. This latter factor is unfortunately very difficult to predict. For tumor surveillance, you will be closely monitored with regularly scheduled office visits in the months and years to follow.
GENERAL POST-OPERATIVE INSTRUCTIONS/CARE
- Activity: Light activity for 1 to 2 weeks is recommended after neck dissection surgery.
- Diet: You can eat a diet as you tolerate after neck dissection, unless throat surgery is performed simultaneously.
- Medicines: You will be prescribed pain medicines and possibly antibiotics. Take these as directed.
- Bathing: Generally, you may shower 24 hours after the drains are removed. Please do not take a bath until one week after your sutures or staples are removed.
- Post-operative follow-up: your sutures or skin clips will be removed 7 to 14 days after surgery. If this post-operative visit has not already been scheduled, please call our office to make that appointment.
At Suburban Ear, Nose & Throat Associates, we take great pride in helping you understand your treatment plan. Care of our head and neck cancer patients is a life-long commitment, and we will develop a long-term relationship of support and careful follow-up. We go to great lengths to try to help you understand your plan of care. If, at any time during your care, you have any questions or concerns, please call us at (847) 259 -2530.
