THYROID CANCER
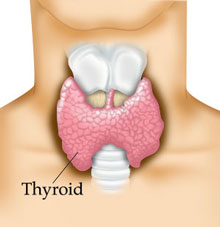
As shown in the diagram, the thyroid gland is a butterfly-shaped organ located in the center of your neck. By secreting thyroid hormone, the thyroid gland controls the metabolism of every cell in your body.
Not infrequently, the thyroid gland develops nodules within it. These nodules are usually identified on routine physical examination, or can be noted on a thyroid ultrasound (a type of imaging). In most cases, thyroid nodules are not tumors, and they do not require surgery. However, thyroid nodules that are found to be tumors will most often require surgery. If the tumor is a benign, only half the gland will need to be removed. This will be diagnosed by a fine needle aspiration (FNA) biopsy. This biopsy is a safe and easy procedure performed with some local anesthesia, either in the office or at the hospital under ultrasound guidance.
There are many types of thyroid cancer, but the three most common include: papillary carcinoma, follicular carcinoma, and medullary carcinoma. In most instances, each of these will require a total thyroidectomy, meaning the entire gland will be removed. Sometimes, a neck dissection will be done in conjunction with the thyroid surgery if there has been any spread of cancer (metastasis) to the adjacent lymph nodes in the neck. Your physician at Suburban Ear, Nose, and Throat has extensive training in both the diagnosis and surgical removal of thyroid cancer.
The postoperative care and risks for thyroidectomy varies whether only a portion of the thyroid gland is to be removed, versus removal of the entire gland. Partial thyroidectomy patients have fewer potential problems after surgery.
2 WEEKS BEFORE SURGERY: Strictly avoid all anti‐inflammatory drugs for two weeks pre‐operatively. This includes aspirin, Advil, ibuprofen, Naprosyn, Celebrex or any other non‐steroidal anti‐inflammatory drug (NSAIDs). These medicines increase your risk of bleeding. These medicines must also be avoided for at least one week after surgery. Tylenol (acetaminophen) is not an anti‐inflammatory so it is fine to take.
NIGHT BEFORE SURGERY: No solid foods (that includes milk, cream etc.) for 8 hours prior to surgery. Typically this means no solid foods after midnight before the surgery. Small volumes of clear liquid may be drank up to 4 hours prior to surgery (examples: water, tea, Gatorade, or coffee with NO milk or cream).
POST‐OPERATIVE CARE: As requested pre‐op, please refrain from aspirin and all NSAID’s for at least 1 week after surgery. We ask that you limit your activity to casual activities for up to 2 weeks. We ask that you do not perform activities that involve lifting more than 15 pounds, excessive bending, stooping, straining, or exercising during this time. We do encourage casual activities such as walking, etc. We encourage taking extra deep breaths every couple hours during the waking hours for a few days after surgery to decrease your risk of post‐operative lung infection. We allow showers 24 hours after your neck drain/drains have been removed. Sutures will typically be removed about seven days after surgery. Sometimes post‐operative antibiotics are prescribed. Narcotic or semi‐synthetic narcotic pain medicine is usually prescribed to be taken on an as needed basis.
DIET: It is typical that we allow you to eat food as tolerated, unless otherwise instructed. Serious complications are rare. It is very important that we are aware if any of the following problems occur. The indications and risks of surgery, as well as expected outcomes, must be understood prior to proceeding with your surgery. In addition, you must understand your alternatives to the surgery. Your alternative is not to have the surgery performed, and continue with medical management of your problem. This would leave you in your current condition.
THYROIDECTOMY SURGICAL RISKS/COMPLICATIONS:
BLEEDING: Minor bleeding from the incision is typically not a problem; however, heavy bleeding deeper in the neck can be very serious and can potentially cause difficulty with breathing. If not addressed in a timely fashion it can possibly cause suffocation. Therefore, if excessive bleeding is noted, if you have sudden difficulty breathing or if there is rapid expansion of your wound, call 911 immediately.
HYPO‐PARATHYROIDISM OR LOW BLOOD CALCIUM: This is a problem that can occur if the entire thyroid gland was removed or if you have had surgery for hyperparathyroidism. You may or may not have been prescribed calcium and vitamin D after surgery. If you develop tingling of your lips, fingers or toes or if your muscles feel spastic or cramping, notify us immediately so this can be also managed in a timely fashion. If this occurs, it is usually temporary, but in rare instances, low blood calcium may be permanent.
HOARSENESS: Thyroid and parathyroid surgery involve dissection around the nerves that control the vocal cords. The vocal cord muscles rotate out to an open position while taking a breath of air and are rotated in and squeezed together in the midline in order to create voice. Each vocal cord has two nerves that control its movement. The larger nerve travels up from below the vocal cords and is named the ‘recurrent laryngeal nerve’. It is responsible for the majority of the movement of the vocal cord. A smaller nerve travels down from above the voice box to control a muscle on the outside of the voice box (larynx). It is named the ‘superior laryngeal nerve’, and it helps in fine tuning the voice allowing for control of your pitch and your ability to project the voice. Surgery to the thyroid or parathyroid places all these nerves at risk for injury. One sided surgery places the upper and lower nerves on that side at risk for injury. Surgery to both sides places all 4 nerves at risk for injury. Permanent damage to these nerves is rare. Temporary injury to these nerves occurs on occasion. The symptoms of laryngeal nerve injury depend on which nerve(s) is affected and can be as minor as mild hoarseness or can be more serious as severe hoarseness. Extremely rarely, if both recurrent laryngeal nerves were to be injured, this could lead to difficulty in breathing in air, necessitating emergency airway control by tracheotomy.
INFECTION: Infection after thyroid is very rare. If there is redness, drainage, fever or other concerns of infection, please notify us immediately.
POSSIBLE NEED FOR FURTHER TREATMENT AND/OR SURGERY: Depending on the problem for which the surgery was performed, as well as the result of the specimens that were sent to the laboratory for pathologic study, sometimes further surgical therapy or further medical therapy is needed. This will be discussed with you by your surgeon.
POOR SCARRING: As Head and Neck Cosmetic and Reconstructive surgeons also, we strive and normally achieve excellent scar camouflage. The scar is typically placed in a previous existing neck crease. Scars are typically raised, somewhat red and bumpy for three months, but over the next year or so, the scar softens, matures and becomes much less visible. Very rarely poor scarring can occur. In these rare instances, scar revision can be performed.
As with any type of surgery, the risks of anesthesia such as drug reaction, breathing difficulties and even death are possible. Please discuss these risks with your anesthesiologist. Fortunately, with this procedure, anesthetic problems are exceedingly rare.
At Suburban Ear, Nose and Throat Associates, Ltd., we go to great lengths to try to help you understand your plan of care. If at any time during your care you have questions or concerns, please call us at 847‐259‐2530.
